
Ethical dilemmas in addiction emergencies often involve life-or-death decisions. Healthcare providers must balance patient autonomy, confidentiality, and resource limitations while navigating biases and legal obligations. Key issues include:
- Patient Autonomy vs. Safety: When patients refuse care after an overdose, providers must decide whether to respect their wishes or intervene to save lives.
- Confidentiality vs. Mandatory Reporting: Privacy laws protect patients, but safety concerns, like child abuse or threats of harm, may require breaching confidentiality.
- Bias in Care: Stigma and prejudice can lead to unequal treatment, affecting vulnerable groups disproportionately.
- Law Enforcement’s Role: Police presence at overdose scenes often deters calls for help, highlighting the need for public health-first response models.
- Resource Allocation: Overcrowded emergency rooms force tough decisions about who gets care first, often influenced by systemic inequities.
Solutions include better training, standardized ethical guidelines, and expanding non-police crisis response models like CAHOOTS. These changes aim to promote fair and compassionate care while addressing systemic gaps.
Common Dilemmas in the Ethical Treatment of Inpatients with Substance Use Disorders
sbb-itb-17645e5
Patient Autonomy vs. Safety in Emergency Responses
When responding to overdoses, healthcare providers often face a tough dilemma: balancing a patient’s right to make their own decisions with the need to provide life-saving care. This tension becomes especially apparent when a patient, revived with naloxone, insists on leaving the scene immediately after regaining consciousness.
Every human being of adult years and sound mind has a right to determine what shall be done with his own body.
In emergencies, patients under the influence of substances may not have the capacity to fully understand or communicate their medical decisions. In such cases, providers often rely on implied consent to proceed with treatment that could save a life.
It’s better to face a judge for having saved a life rather than allow a person to die untreated for an easily treated condition.
Naloxone’s effects are short-lived, while the opioids it reverses can linger in the body for hours. This creates a dangerous window where refusing further care could lead to a secondary overdose.
When Involuntary Treatment Is Justified
In many states – 37 plus Washington, D.C. – laws permit involuntary treatment when a person poses a clear risk to themselves or others. This is often based on criteria such as being “gravely disabled” or presenting a “likelihood of serious harm” . For instance, California’s Bill 43, passed in October 2023, expanded these criteria to allow conservatorship for individuals whose substance use prevents them from meeting basic needs. Under the legal principle of parens patriae, the government steps in to protect those unable to protect themselves, but this is typically seen as a last resort .
However, there are risks tied to forced treatment. For example, abstinence during involuntary care lowers drug tolerance, which can make relapse particularly dangerous. Statistics show that about one-third of patients relapse on the very day they are discharged from mandated treatment, increasing the risk of fatal overdose.
These laws underscore the delicate balance between respecting autonomy and ensuring safety.
Obtaining Consent in Crisis Scenarios
Determining whether a patient can provide informed consent during a crisis is rarely straightforward. While some facilities use specific measures like a blood alcohol threshold of 80 mg/dL, most physicians rely on their clinical judgment. Tools such as the Aid to Capacity Evaluation (ACE) can help assess whether a patient understands the risks, aligns their decisions with personal values, and can explain their reasoning.
It’s also important to note that intoxicated patients generally cannot refuse life-saving treatments. For example, someone may be required to undergo a mental health evaluation for suicide risk, even if they can decline less urgent care like cosmetic sutures. Providers must carefully document any refusal of care. This includes confirming that the patient is aware of the life-threatening risks and recording their response.
Roughly 5% to 10% of emergency medical calls end with patients refusing transport. In such cases, thorough documentation is critical. Using standardized “high-risk refusal” checklists and consulting online medical oversight can help ensure that ethical and legal responsibilities are met.
Confidentiality vs. Mandatory Reporting in Addiction Crises
When dealing with addiction crises, healthcare providers often face a delicate balancing act between respecting patient privacy and fulfilling legal reporting requirements. Under federal regulations like 42 C.F.R. Part 2, addiction treatment programs are prohibited from disclosing patient-identifying information without consent. However, these protections are not absolute – situations involving safety concerns can override confidentiality rules.
This conflict becomes especially challenging in cases such as suspected child abuse, threats to harm others, or imminent suicide risks. In such instances, legal obligations take precedence. For example, all states require professionals to report known or suspected child abuse or neglect. Additionally, in 27 to 33 states, there are laws mandating that providers warn third parties if a patient poses a specific threat to someone’s safety [23, 24].
“The general requirement that counselors keep information confidential does not apply when disclosure is required to protect clients or identifiable others from serious and foreseeable harm or when legal requirements demand that confidential information be revealed.”
These legal mandates are not just theoretical – they have real-world consequences. In one study, parental substance use was the sole reason for removing children under one year old from their homes in 16.6% of cases and a contributing factor in 50.8% of cases. Moreover, 46 states impose criminal penalties on professionals who fail to report child abuse, with potential fines or license revocation for non-compliance.
Legal and Ethical Implications of Mandatory Reporting
Mandatory reporting laws rely on a “reasonable suspicion” standard, meaning providers do not need conclusive proof to file a report. This standard is intended to err on the side of caution, prioritizing the safety of vulnerable individuals.
Federal confidentiality rules under 42 C.F.R. Part 2 include a narrow exception for reporting child abuse or neglect. While providers can make the initial report as required by state law, they cannot respond to follow-up requests or subpoenas without the patient’s written consent.
“The child abuse reporting exception applies only to initial reports of child abuse or neglect (42 C.F.R. §2.12 (c)). Programs may not respond to follow-up requests for information or to subpoenas for additional information… without the client’s written consent.”
- Substance Abuse and Mental Health Services Administration (SAMHSA) [24, 28]
To encourage compliance, professionals who report in “good faith” are typically granted immunity from civil or criminal liability. This legal protection helps ease the burden of breaching confidentiality, though it doesn’t eliminate the ethical challenges of breaking trust with patients [24, 28].
It’s worth noting that substance use alone does not automatically trigger a mandatory report. Many states require evidence that substance use has led to actual harm, such as neglect or failure to meet a child’s basic needs.
Clear communication before a crisis arises is key to managing the tension between privacy and reporting requirements.
How to Balance Privacy and Legal Obligations
The best way to navigate these challenges is to establish clear expectations from the beginning. During intake, providers should explain the limits of confidentiality, emphasizing that threats of harm or suspected abuse must be reported by law [24, 26].
“Addiction professionals, during informed consent, shall disclose the legal and ethical limits of confidentiality and shall disclose the legal exceptions to confidentiality.”
When making a report, providers should limit disclosures to the essential details required by state law, such as the patient’s name, address, and the type of abuse. Additional records should not be released without the patient’s explicit consent or a court order.
Maintaining transparency with the patient can also help preserve trust. When appropriate, providers can inform patients that a report is being made and even involve them in the process, such as allowing them to be present during the call to authorities [24, 27]. This collaborative approach can help mitigate feelings of betrayal.
In situations that are less clear-cut, consultation is crucial. Providers should seek guidance from a clinical supervisor, peer, or legal counsel to ensure that the “reasonable suspicion” standard is met and that the response aligns with the level of risk [24, 26]. Not every concern requires immediate reporting; some issues may be better managed through closer monitoring or enhanced counseling.
Finally, thorough documentation is essential. Providers should keep detailed records of informed consent discussions, observations leading to the report, and any consultations that influenced the decision. This not only protects the provider but also ensures that patient care remains a priority throughout the process [27, 31].
Law Enforcement Collaboration During Overdose Emergencies
Public Health vs Policing Approaches to Overdose Emergencies
Overdose emergencies often bring together medical responders and law enforcement, creating a complex mix of priorities. While police are frequently part of 911 responses, their focus on maintaining public order can sometimes shift the situation from a medical emergency to a criminal matter. This dynamic raises significant ethical concerns.
In a nationwide survey, 36% of police officers reported making arrests at overdose scenes. This arrest rate generates fear among bystanders, discouraging them from calling 911 when every second is critical. The result? Fewer timely calls for help and missed opportunities to save lives.
Good Samaritan laws aim to protect those who call 911 during an overdose, but they often exclude individuals on probation, parole, or with active warrants. These gaps in protection erode trust in the system and leave many hesitant to seek help in emergencies.
Another pressing issue is the sharing of overdose data between health agencies and law enforcement. In some areas, this information is used for activities like door-knocking follow-ups or investigations into drug-related homicides, effectively creating lists of individuals who use drugs. Such practices can lead to coercive treatment, which has been linked to higher rates of relapse and overdose.
Public Health vs. Policing Approaches
The tension between traditional policing and public health-focused responses becomes clear when comparing their priorities and outcomes:
| Feature | Policing-Led Response | Public Health-Focused (e.g., CAHOOTS) |
|---|---|---|
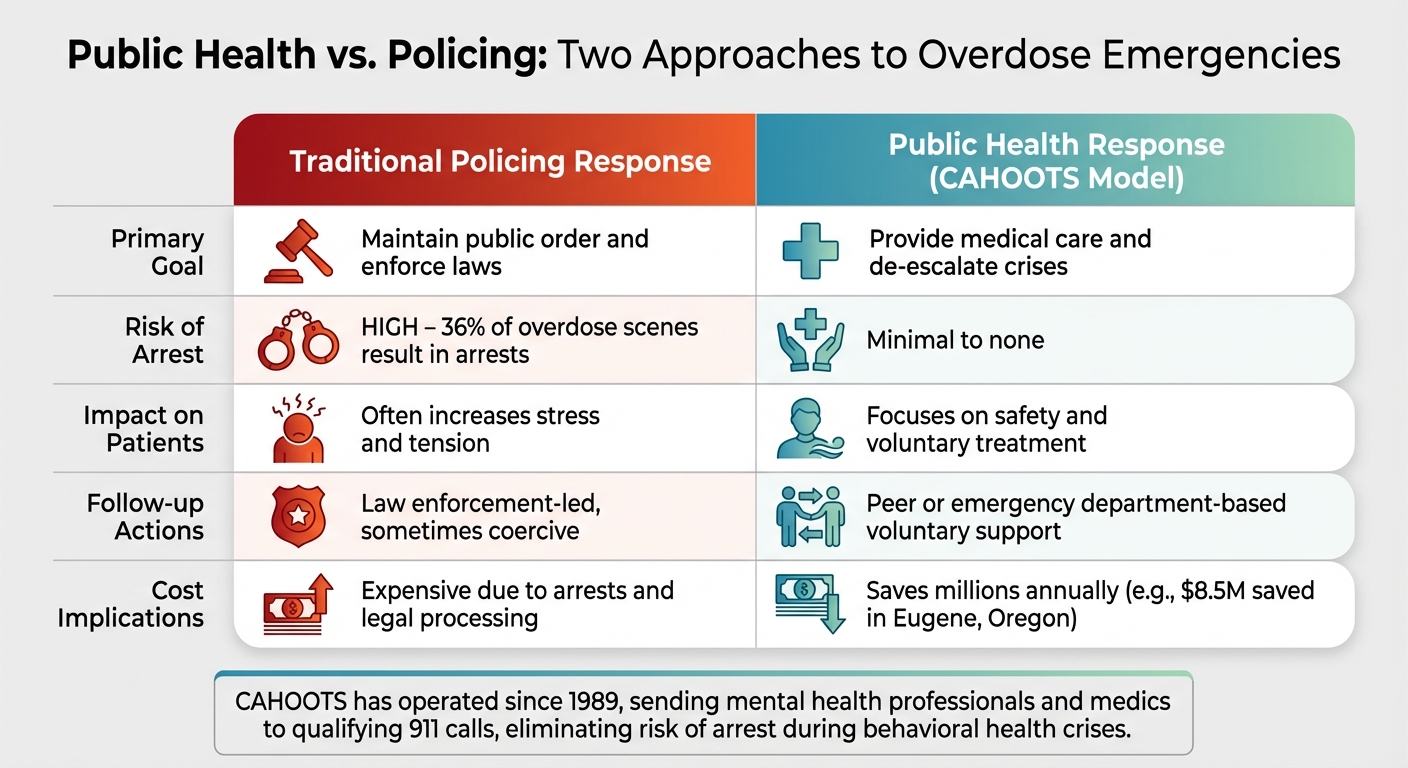
| Primary Goal | Maintain public order and enforce laws | Provide medical care and de-escalate crises |
| Risk of Arrest | High – 36% of overdose scenes result in arrests | Minimal to none |
| Impact on Patients | Often increases stress and tension | Focuses on safety and voluntary treatment |
| Follow-up Actions | Law enforcement-led, sometimes coercive | Peer or emergency department-based voluntary support |
| Cost Implications | Expensive due to arrests and legal processing | Saves millions annually (e.g., $8.5M in Eugene, Oregon) |
Programs like CAHOOTS in Eugene, Oregon, demonstrate the potential of a public health-first approach. Since 1989, CAHOOTS has sent mental health professionals and medics to handle qualifying 911 calls, bypassing the need for police intervention. The program not only eliminates the risk of arrest or police violence during behavioral health crises but also saves an estimated $8.5 million annually in public safety costs. Inspired by CAHOOTS, other cities like Denver, New York, and San Francisco are adopting similar models, supported by federal funding through the 2021 American Rescue Plan.
“The pattern toward criminalizing our response to behavioral health crises is unmistakable, unsustainable, and counterproductive.”
- Amy L. Solomon, Department of Justice’s Office of Justice Programs
Shifting overdose responses to align with public health priorities could save lives, reduce costs, and rebuild trust in emergency systems.
Bias and Resource Allocation in High-Demand Situations
Picture this: an overcrowded emergency room, limited resources, and a critical decision about who gets care first. Ideally, medical need should dictate these choices. But in reality, bias – whether tied to race, income, or addiction stigma – often sneaks into the equation, influencing decisions in ways that stray far from fairness.
The ethical principle of justice calls for equal treatment for patients with similar medical needs. Yet, this principle is frequently undermined when prejudice clouds clinical judgment. For instance, a homeless individual struggling with addiction might be sent to a shelter with a basic outpatient appointment, while someone with identical psychiatric symptoms – but with influential connections, like being the child of a hospital benefactor – receives more comprehensive care. Dr. Adam Bernstein of SUNY Upstate Medical University highlights this as a clear violation of justice.
These disparities aren’t just theoretical; the numbers paint a stark picture. Black patients with substance use disorders are 53% less likely to be assigned an immediate or emergent triage level compared to White patients with the same condition. They also face an 18.5% higher risk of being under-triaged in emergency departments. This double stigma results in longer wait times and fewer interventions for Black patients.
Financial barriers make matters worse, especially in addiction emergencies. In states like Kentucky, Ohio, and Utah, a “pledge of financial commitment” is required before a judge will approve involuntary commitment for treatment. This effectively shuts out patients without the means to pay, leaving many without access to life-saving care. In 2022, only 26% of the 48.7 million Americans diagnosed with a substance use disorder received any form of treatment.
Clinicians’ biases also play a role. Patients perceived as “drug-seeking” or displaying behaviors like impulsivity or dishevelment often face stigma that influences care decisions. Dr. Laura Weiss Roberts from Stanford University stresses the importance of professionalism, urging providers to seek therapeutic approaches while setting aside prejudicial attitudes.
Ethical Triage in Addiction Emergencies
Addressing these inequities requires rethinking how emergency departments manage triage. Right now, subjective clinical judgment dominates the process, leaving room for bias to creep in. Research shows that about one-third of emergency department visits are mistriaged due to this subjectivity.
One solution lies in standardizing triage protocols. Tools like the Emergency Severity Index (ESI) can be modified to include objective criteria, reducing the likelihood that marginalized groups are under-triaged. Dr. Priyanka Amin from the University of Pittsburgh School of Medicine urges providers to critically examine how bias affects their perceptions, particularly in cases involving agitation or the use of restraints.
Training programs that focus on cultural humility and implicit bias can also make a difference. Unlike traditional “checklist” approaches to cultural competency, these programs encourage self-reflection and an understanding of power dynamics, helping providers address both explicit and implicit bias. Skills like motivational interviewing can further enhance these efforts.
Another strategy is adopting a “No Wrong Door” policy. This ensures that patients, regardless of whether they seek help through mental health, addiction, or emergency services, receive an initial assessment and appropriate referrals. Care coordination models, such as Nurse Care Managers or Medicaid health homes, streamline patient care by organizing activities and sharing information across providers. This not only improves patient engagement but also helps reduce costs.
For vulnerable populations, outreach efforts must meet people where they are – whether that’s in their homes or in community spaces they trust. The COVID-19 pandemic highlighted a “digital divide”, where low-income or homeless patients lacked access to the technology needed for telehealth services. Bridging this gap means addressing these technological barriers and offering flexible service options to ensure no one is left behind.
Policy Reforms for Ethical Emergency Planning
The challenges discussed earlier highlight systemic gaps that demand real policy changes. Without clear frameworks, responders often face life-or-death decisions with inconsistent guidance. Addressing these gaps through policy reforms can ensure ethical and consistent emergency care.
Training and Standardized Guidelines for Ethical Care
Currently, most U.S. states only require 2 to 6 hours of ethics training every two years for addiction counselors to maintain their credentials. That’s hardly enough to prepare professionals for the complex ethical dilemmas they encounter.
“Because of the highly charged emotional nature of the substance abuse treatment field, providers should possess the tools to explore ethical dilemmas objectively.” – Substance Abuse and Mental Health Services Administration (SAMHSA)
Effective training should go beyond compliance. It can reshape how responders understand addiction, framing it as a treatable disorder rather than a moral failing. This shift reduces bias in care. Training also equips responders with a framework rooted in principles like Justice, Autonomy, and Beneficence, helping them make decisions based on ethics rather than emotion.
Adopting national model standards for licensure based on The ASAM Criteria can ensure patients receive care that aligns with ethical standards. Standardizing these guidelines across states would create consistency. Additionally, aligning state privacy laws with federal 42 CFR Part 2 could ease care coordination and promote the use of electronic health records during emergencies.
Expanding Non-Police Crisis Response Models
The limitations of traditional law enforcement in addiction-related emergencies make a strong case for alternative approaches. Sending police to handle these crises often escalates risks and fails to connect individuals with appropriate treatment. For example, individuals showing signs of mental illness during police encounters face a death rate of 20 per million, compared to 3 per million for those without such signs.
Public health-led crisis response models offer a safer and more compassionate alternative. Programs like Crisis Assistance Helping Out on the Streets (CAHOOTS) in Eugene, Oregon, dispatch a paramedic and crisis worker to handle calls involving mental health or addiction. This approach successfully diverts individuals from police custody to medical care. Such models not only reduce criminalization but also align with the ethical principles of care discussed earlier.
Another example is the initiative launched by Police Chief Leonard Campanello in Gloucester, Massachusetts, in June 2015. People with substance use disorders could turn in drugs or equipment at the police station without facing charges. Instead, they were paired with “angel” volunteers who guided them through detox and recovery. This approach treats addiction as a health issue rather than a criminal offense.
The 988 Suicide & Crisis Lifeline is another promising tool. Local governments could pilot programs allowing 911 dispatchers to transfer non-violent addiction-related calls directly to 988-led mobile crisis teams. This reform is crucial given that 68% of jail inmates have a diagnosable substance use disorder, yet fewer than 15% receive treatment while incarcerated.
| Model Type | Primary Responders | Role of Law Enforcement |
|---|---|---|
| Crisis Intervention Team (CIT) | Specially trained police officers | Lead responders; coordinate with providers |
| Co-Responder Team (CRT) | Police officer + Mental health clinician | Joint response in the field |
| Mobile Crisis Team (MCT) | Community-based mental health professionals | Called in only when safety concerns arise |
| 988 Lifeline | Trained crisis counselors | Remote support; can deploy MCTs |
Scaling these models will require funding and political commitment, but the benefits are clear. For instance, care coordination models like Nurse Care Managers have shown success in improving patient engagement and cutting costs by streamlining communication between providers. Policies that allow for increased “take-home” methadone doses during emergencies and relax strict drug screening requirements also ensure continuity of care when it’s most critical.
Conclusion: Ensuring Ethical Care in Addiction Emergencies
Responding to addiction-related emergencies presents complex ethical challenges for healthcare professionals. With over 70,000 overdose deaths occurring annually in the U.S. and only 26% of individuals with substance use disorders receiving treatment, decisions about autonomy, confidentiality, and resource allocation carry immense weight – often determining life or death outcomes.
Emergency departments are legally bound by EMTALA to provide evidence-based care, including medications for opioid use disorder and naloxone distribution. Failing to implement these practices may also breach the Americans with Disabilities Act.
“This report adds to the professional consensus that providing effective addiction care in the emergency department is an obligation, not an option.” – Joshua Sharfstein, MD, Director, Bloomberg American Health Initiative
This legal and ethical responsibility highlights the pressing need for improved training and policy reforms. Current training requirements, often limited to 2–6 hours every two years, must be expanded to include comprehensive ethical decision-making frameworks like The ASAM Criteria. Such training equips responders to handle nuanced situations – balancing patient autonomy with safety concerns, managing confidentiality alongside mandatory reporting, and distributing limited resources fairly when demand exceeds availability. Additionally, integrating non-police crisis response models, as previously discussed, strengthens this approach to care.
Shifting the focus from criminalization to health-centered strategies – through harm reduction, standardized ethical guidelines, and pathways to treatment – offers a more effective response to addiction emergencies. These measures not only save lives but also ensure responders consistently provide ethical, compassionate care.
For more information on treatment options and recovery resources, visit Sober Living Centers.
FAQs
When can providers treat someone who refuses care after naloxone?
Providers can treat individuals who decline care after receiving naloxone, but only if they meet specific safety criteria and are judged capable of making informed decisions. Research indicates that mortality rates in such cases are extremely low – ranging from 0% to 0.48% – within 24 to 28 hours following refusal. This suggests that, in certain situations, delaying treatment may be a safe option.
What breaks confidentiality in an addiction emergency?
In addiction emergencies, confidentiality might need to be set aside to prioritize safety. This can happen in cases involving risks like abuse, violence, suicidal behavior, or when legal obligations demand disclosure. The focus in such situations is on safeguarding individuals while adhering to legal requirements.
How can ERs reduce bias when triaging overdose patients?
Emergency Rooms (ERs) can help minimize bias by implementing algorithmic triage decision support systems that rely on standardized criteria, such as the Emergency Severity Index (ESI). By using these systems, ERs can tackle ethnoracial disparities and ensure a more equitable approach to prioritizing care, particularly for overdose patients.

