
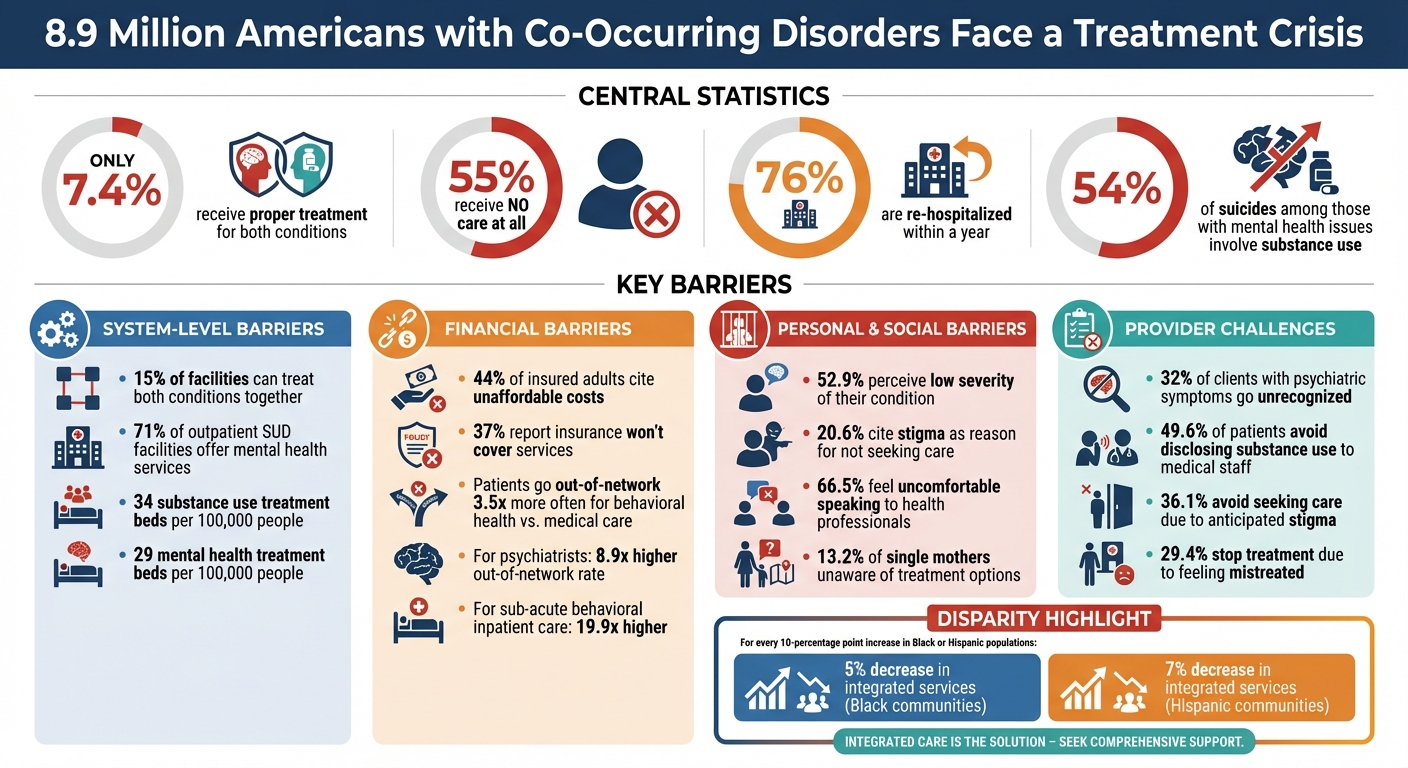
The U.S. faces a severe crisis in addressing mental health and substance abuse, particularly for the 8.9 million adults with co-occurring disorders (both mental health and substance use issues). Despite the urgent need, only 7.4% receive proper treatment for both conditions, while 55% get no care at all. Key barriers include:
- Limited access to integrated care: Only 15% of facilities can treat both conditions together.
- Financial obstacles: High costs and poor insurance coverage prevent many from seeking help.
- Stigma: Fear of judgment discourages individuals from pursuing treatment.
- Provider challenges: Workforce shortages, lack of training, and biases hinder effective care.
These issues are compounded by systemic disparities, particularly in rural and minority communities. Solutions like integrated care models, better workforce training, and policy reforms are essential to close the treatment gap and improve outcomes.
Mental Health and Substance Abuse Treatment Gap Statistics
Dual diagnosis of mental illness and substance use disorder
sbb-itb-17645e5
System-Level Barriers to Treatment Access
The United States faces a significant gap in the infrastructure needed to treat co-occurring mental health and substance use disorders. Shockingly, only 15% of facilities are equipped to address both issues simultaneously. Nationwide, there are just 34 substance use treatment beds and 29 mental health treatment beds per 100,000 people, leaving many individuals waiting weeks or even months for care – if it’s available at all.
Not Enough Treatment Services
The lack of treatment capacity is compounded by a shortage of specialized centers, leaving millions without proper access to care. While 83% of substance use facilities offer outpatient services, only 7% provide intensive inpatient care. Adding to the challenge, most integrated facilities are located in large metropolitan areas like Minneapolis, Chicago, Atlanta, and New York, making access even harder for those in rural regions.
In communities with higher Black or Hispanic populations, the situation is even worse. For every 10-percentage point increase in these demographics, the likelihood of a facility offering integrated services drops by 5% and 7%, respectively.
"Access to integrated mental health services within SUD outpatient treatment facilities was disproportionately lower in communities that were predominately Black and Hispanic" – George Pro, University of Arkansas for Medical Sciences
This uneven distribution of resources has turned many minority-dense areas into treatment deserts, where finding help becomes nearly impossible.
Treatment Costs and Insurance Problems
Even when services are available, financial barriers prevent many from getting the care they need. Among insured adults who didn’t receive mental health care, 44% cited unaffordable costs, while 37% reported that their insurance wouldn’t cover the necessary services.
Behavioral health providers are systematically underpaid compared to other medical specialists, which creates a network problem. Providers may appear in-network but often don’t accept insurance in practice. The disparity in reimbursement is stark – on average, in-network office visits for medical/surgical clinicians are reimbursed 22% more than those for behavioral health clinicians. At higher claim levels, this gap can soar to 70%.
This financial imbalance forces patients to seek out-of-network care far more often for behavioral health services. For example:
- Patients go out-of-network 3.5 times more often for behavioral health services compared to medical care.
- For psychiatrists, this rate jumps to 8.9 times higher.
- For sub-acute behavioral inpatient care, the difference skyrockets to 19.9 times higher than for medical inpatient care.
Policy and Legal Obstacles
Regulatory challenges further complicate access to integrated care. Licensing requirements differ significantly between mental health and substance use professionals. While mental health providers typically need a master’s degree, substance abuse counselors often require only a bachelor’s degree or less. This disparity reinforces the separation of mental health and substance use treatment, perpetuating a fragmented system.
Privacy laws, such as 42 CFR Part 2, also create roadblocks. These regulations prevent the inclusion of substance use data in general electronic health records, making it difficult for providers to coordinate care.
"Integration of SUD treatment services across general or mainstream health care systems can help address the misuse of substances and related consequences, reducing health disparities, saving costs, and meeting the needs of people with SUDs" – Substance Abuse and Mental Health Services Administration (SAMHSA)
However, current policies make this integration both legally and administratively challenging. On top of that, the fear of criminal justice repercussions discourages many patients from disclosing substance use in healthcare settings. These systemic hurdles contribute to the persistent gaps in treatment for those with co-occurring disorders.
Personal and Social Barriers to Getting Help
While systemic challenges make accessing treatment for co-occurring disorders difficult, personal and social factors add another layer of complexity. These obstacles – ranging from stigma to unsupportive environments – often prevent individuals from seeking or continuing care.
Stigma and Shame
Stigma is a powerful barrier, operating on both societal and personal levels. Public stigma, or society’s negative perceptions of addiction and mental illness, can lead to discrimination in areas like housing, employment, and social relationships. On the other hand, self-stigma occurs when individuals internalize these negative attitudes, viewing themselves as undeserving of help or seeing their struggles as moral failings rather than health issues.
"Addiction is one of society’s most misunderstood and rebuked health conditions. That stigma discourages many people from seeking treatment for substance dependence." – Anne C. Krendl, Psychological Scientist, Indiana University
Substance use disorders often face harsher judgment than mental health conditions because they’re seen as "controllable." This judgment contributes to a reluctance to seek help; for instance, in a global survey, 20.6% of people who recognized a need for care but didn’t pursue it cited stigma as the main reason. Women with co-occurring disorders face additional challenges, fearing labels like "unfit mother" and potential involvement from Child Protective Services, which creates even more shame and hesitancy.
Stigma doesn’t just delay treatment – it can also lead to premature dropout, as individuals try to avoid judgment from healthcare providers or their community.
Not Knowing About Treatment or Feeling Ready
Many people underestimate the seriousness of their condition. In fact, 52.9% of individuals with diagnosed disorders reported "low perceived severity" as their reason for not seeking treatment. They may believe their situation will improve on its own or think they should handle it without professional help.
Even when someone realizes they need care, gaps in knowledge can be a significant hurdle. For example, 13.2% of single mothers were unaware of available treatment options, and 43.7% assumed their insurance wouldn’t cover behavioral health services.
Psychological readiness also plays a major role. In Colorado, 66.5% of individuals skipped needed substance use treatment because they felt uncomfortable speaking to a health professional. This discomfort is especially common among younger adults (ages 18–30), with 82.8% citing it as a concern, compared to 59.4% of those aged 31–49. While recognizing the need for treatment increases the likelihood of receiving care by about tenfold, only about one-third of those individuals actually seek help.
Family, Friends, and Environment
External factors, including relationships and living conditions, can also block access to treatment. Family members and friends can be both a support system and a source of resistance. Caregivers, for instance, report growing difficulties navigating fragmented healthcare systems, with challenges like insufficient childcare and time constraints rising from 23% in 2015 to 31% in 2020 – and up to 45% for those managing mental health care.
Unsupportive family dynamics can be particularly harmful. Single mothers, for example, often avoid disclosing substance use or mental health issues out of fear of losing custody of their children. Social networks can further complicate matters when they provide conflicting advice or discourage individuals from following clinical recommendations.
Environmental challenges also play a role. Limited transportation options in rural areas, unstable housing, and the lack of private spaces for virtual therapy can make it harder to maintain consistent care. Additionally, family and friends may dismiss clinical symptoms, labeling anxiety as "worrying too much" or depression as "laziness", which can prevent individuals from recognizing these issues as legitimate health conditions that require treatment.
Challenges Healthcare Providers Face
Healthcare providers encounter numerous hurdles when it comes to delivering comprehensive care for individuals with co-occurring disorders. These challenges range from resource limitations and workforce shortages to training deficits and ingrained biases.
Limited Resources and Staffing
The healthcare infrastructure in the U.S. often falls short in addressing the needs of dual-diagnosis patients. For example, only 71% of licensed outpatient substance use disorder treatment facilities offer integrated mental health services. That leaves nearly 30% of facilities unequipped to manage both conditions at the same time. The problem is even worse in specialized care settings – residential rehabilitation programs and intensive inpatient units for co-occurring disorders are scarce, leading to long waitlists.
Staffing shortages exacerbate these issues. Many facilities lack case managers trained in handling dual diagnoses, and there aren’t enough clinicians with DEA waivers to prescribe medication for opioid use disorder. High caseloads and the pressure to meet billing targets make it difficult for staff to pursue additional training. As one social worker shared:
"There’s a lot of emphasis on our productivity. When we’ve asked for things like trainings, we’ve gotten [the response from management] ‘You guys are underperforming’"
.
Fragmented systems also contribute to the problem. Mental health and substance use services often operate in separate administrative and financial silos, making it harder to coordinate care. Geographic disparities further complicate access – communities in the South, Midwest, and Mountain West generally have fewer integrated care options compared to large metropolitan areas in the Eastern U.S. Additionally, research shows that for every 10-percentage point increase in a community’s Black population, the odds of a facility offering integrated services drop by 5%, with a 7% decrease for Hispanic populations.
These structural issues not only limit resources but also hinder the ability of providers to receive adequate training, perpetuating biases and gaps in care.
Training and Knowledge Gaps
A lack of specialized training leaves many healthcare professionals unprepared to manage the complexities of co-occurring disorders. For instance, counselors failed to identify the need for mental health services in 32% of clients who reported psychiatric symptoms, even though 36% of those clients explicitly requested help. This reflects a systemic shortfall in training, which prevents providers from effectively addressing dual diagnoses.
Without integrated expertise, patients frequently find themselves caught in a frustrating loop – mental health services direct them to substance use teams, while substance use teams defer to mental health services. As one social worker described:
"I assess people in crisis who use alcohol or drugs to cope with distress, but trying to get them into mental health services is near impossible. They’re told to work with substance use teams first, but those teams don’t deal with their mental health"
.
Some providers also enforce "abstinence-first" policies, denying mental health treatment until patients are sober. For individuals using substances to cope with distress, this approach can be counterproductive. The mismatch between training and patient needs often leads to burnout among providers. One community psychiatric nurse shared their experience:
"I have three CEMS patients on my caseload of 40. They take all of my time. I often go home at night thinking tomorrow will be the day one of them is found dead. It’s exhausting"
.
Provider Bias and Reluctance
Bias within the healthcare system further undermines patient care and engagement. Between September 2021 and August 2024, researchers at the University Hospital Frankfurt found that nearly half (49.6%) of adult inpatients with substance use disorders avoided disclosing their substance use to medical staff, fearing they would receive worse treatment. Additionally, 36.1% of patients avoided seeking medical care due to anticipated stigma, and 29.4% stopped treatment because they felt mistreated for their addiction.
Many healthcare providers still view addiction as a moral failing rather than a medical condition, leading to dismissive or even hostile interactions. This bias can result in misdiagnosis or neglect of co-occurring conditions. A dual diagnosis link worker explained:
"When I get someone who drinks or uses drugs and is mentally unwell, I tell them not to tell mental health services they use substances, because I know they won’t get the support they need"
.
These biases are often compounded for patients with intersecting stigmatized identities. A study of care management staff in Boston Medical Health System‘s Medicaid accountable care organizations highlighted significant disparities affecting Latine patients. For example, one Latine patient on dialysis waited over two weeks for a treatment appointment through a federal helpline, while a non-Latine patient received immediate care for alcohol use disorder after being released from incarceration. Reflecting on these inequities, a community health worker noted:
"It takes more to bring Latina women into any kind of help (for SUD) because they have kind of taken in that shame"
.
Addressing these systemic challenges is essential to bridging the gaps in care for individuals with co-occurring disorders.
Research Findings and Ways to Improve Access
Summary of Barriers and What Helps
Research reveals a staggering treatment gap for the 8.9 million American adults living with co-occurring disorders. Only 7.4% receive care for both conditions, and a troubling 55% receive no treatment at all. The barriers to care can be grouped into three interconnected categories.
System-level challenges include a lack of integrated services – just 71% of licensed outpatient substance use disorder facilities provide mental health services as well. Other hurdles include long wait times, complex enrollment procedures, and high costs. Geographic and racial disparities compound the problem, with minority-dense areas often having fewer integrated care options.
Personal and social obstacles also play a major role. Stigma, lack of awareness about available resources, and practical issues like transportation and childcare prevent many from seeking help. Notably, individuals who recognize their need for treatment are about ten times more likely to receive care compared to those who don’t.
Provider-level issues complete the picture. These include insufficient training on co-occurring disorders, workforce shortages, and biases within the system. However, research highlights several factors that make a difference: family support, peer-recovery specialists, accessible care options, and integrated treatment models that address both conditions in tandem. These findings emphasize the urgency of implementing practical solutions, as outlined below.
Recommendations for Better Treatment Models
Experts suggest adopting integrated care frameworks like Integrated Dual Disorder Treatment (IDDT) and Certified Community Behavioral Health Clinic (CCBHC) models. IDDT relies on multidisciplinary teams – including peer-recovery specialists, behavioral health experts, and pharmacists – to deliver comprehensive, ongoing support and proactive outreach. Meanwhile, the CCBHC model uses bio-psychosocial approaches to provide holistic care.
To make these models viable, licensing and reimbursement processes need to be streamlined. Financial incentives are crucial to offset the high costs of integrated care, such as expanding insurance coverage and reforming payment systems to allow providers to bill for both substance use and mental health services simultaneously.
Workforce development is another pressing need. The Extension for Community Healthcare Outcomes (ECHO) model has proven effective in equipping providers with the skills to manage complex cases and prescribe treatments like buprenorphine. Increasing addiction medicine education for medical and nursing students, along with offering ongoing training and expert supervision for current providers, addresses critical training gaps. This is especially important given that 32% of clients with psychiatric symptoms go unrecognized. Routine mental health screenings and patient education can also improve treatment readiness. Combining policy reform with local community resources is essential for narrowing the treatment gap.
Accessible educational platforms are another key strategy for addressing these systemic issues.
How Sober Living Centers Can Help
Navigating the fragmented treatment landscape can feel overwhelming. Sober Living Centers offers educational resources that tackle many of the knowledge gaps identified in research. Their website provides detailed guides on the importance of integrated care, which is widely regarded as the gold standard for treating co-occurring substance use and mental health disorders. These guides help individuals and families understand what to look for in a treatment facility.
The materials also offer practical advice on selecting programs with multidisciplinary teams, diverse therapy options, and strong aftercare support. For families who have experienced past treatment failures or feel daunted by the complexities of dual diagnosis, these resources serve as a valuable starting point. By breaking down the causes, symptoms, prevention strategies, and treatment options for co-occurring disorders, Sober Living Centers helps close the knowledge gap that often prevents people from seeking care. These educational tools align closely with the integrated treatment models recommended by experts.
Conclusion
The challenges keeping 8.9 million Americans with co-occurring disorders from accessing care go far beyond paperwork – they’re life-threatening. With only 7.4% receiving treatment for both conditions and over half receiving no treatment at all, the stakes are dire. Numbers tell the story: 76% of these individuals are re-hospitalized within a year, and substance use plays a role in 54% of suicides among those with mental health issues.
Addressing these challenges demands action on multiple fronts. At the system level, the fragmented funding and billing structures need to be overhauled. These outdated frameworks force providers to choose between treating mental health or substance use, leaving patients stuck in a cycle of fragmented care with no accountability. On a societal and personal level, eliminating harmful stigma is just as important. Viewing substance use as a trauma response rather than a moral failing and removing abstinence-based barriers that trap people in a "Catch-22" are crucial steps forward.
"Structural reform is not merely a technical issue, but a moral and political imperative – one that must centre lived experience, dismantle systemic stigma, and reimagine service design through the lens of justice and dignity." – Discover Public Health
Solutions are within reach, and research points to what works: integrated care models, improved workforce training, policy changes, and accessible educational tools can bridge the gap between needing help and receiving it.
Real progress happens when policymakers, healthcare professionals, families, and individuals collaborate to create a system where no wrong door exists – a system where anyone seeking help can find comprehensive, integrated care no matter where they start. The time to act is now.
FAQs
What is integrated treatment for co-occurring disorders?
Integrated treatment for co-occurring disorders takes a coordinated approach, tackling mental health conditions and substance use disorders at the same time. By offering care that’s trauma-informed and focused on individual needs, this method minimizes fragmented services and helps achieve better results for those receiving treatment.
How can I find dual-diagnosis care if I live in a rural area?
Accessing care for dual-diagnosis in rural areas can be tough because resources are often scarce. However, there are ways to navigate these challenges. Telehealth services offer a convenient solution by connecting patients with specialists remotely, removing the need for long-distance travel. Additionally, treatment locators provided by government agencies can help pinpoint nearby programs.
Many healthcare facilities are now combining mental health and substance use treatment within their existing services, simplifying access for patients. Reaching out to local healthcare providers or national helplines can also lead you to personalized support options tailored to your needs.
What can I do if my insurance won’t cover mental health or addiction treatment?
If your insurance doesn’t include mental health or addiction treatment, there are still ways to seek support. You can start by reaching out to specialized helplines that offer guidance on available resources. Another option is to advocate for changes in insurance policies to improve coverage. Exploring out-of-network providers is also worth considering, though it’s important to note that this might come with higher costs or longer wait times. Additionally, taking advantage of educational resources can help you better understand treatment options and recovery strategies.

